Healthcare
How a Multi-Specialty Healthcare Group Reduced Prior Authorization Delays and Administrative Burden with an AI Workflow System
A mid-sized specialty care group in Southern California with multiple locations across
cardiology, imaging, and outpatient procedural care.
The Challenge
The client was struggling with prior authorization.
Their clinical and administrative teams were spending too much time gathering records, checking payer requirements, submitting documentation, responding to requests for more information, and following up on delayed or denied authorizations.
The workflow was highly manual and spread across multiple systems:
The EHR
Payer portals
Fax and PDF attachments
Internal work queues
Staff notes and spreadsheets
As volume increased, the problem became harder to manage. The organization was dealing with:
- Delayed authorizations for imaging and procedures
- Repeated manual collection of clinical documentation
- Staff spending hours each week chasing status updates
- Inconsistent submission quality across payers
- Denials caused by missing or incomplete information
- Growing frustration from both staff and patients
This aligns closely with the broader industry reality you researched: prior authorization is one of the most painful and repetitive workflows in healthcare, with high volumes, heavy manual work, fragmented systems, and direct downstream care delays.
The Business Impact
This was not just an administrative inconvenience. Prior authorization delays were affecting
Patient scheduling
Clinician workflows
Staff capacity
Reimbursement timing
Patient satisfaction
Our Approach
We did not start by building an AI tool. We started by analyzing the full prior authorization workflow from the moment an order was placed to the moment the authorization was approved, denied, or escalated.
That work included:
Stakeholder interviews with operations leaders, authorization staff, and clinical teams
Mapping the differences between payer workflows
Reviewing how staff gathered supporting clinical evidence
Identifying where information was re-entered or reformatted
Analyzing the most common causes of rework, delays, and denials
Defining where human review needed to stay in place
- The evidence lived in one place
- The payer requirements lived in another
- The submission process happened through multiple external channels
- Staff were forced to keep the workflow together manually
That matches the research pattern: healthcare organizations spend disproportionate time on
“proof work” and manual workflow coordination across disconnected systems.
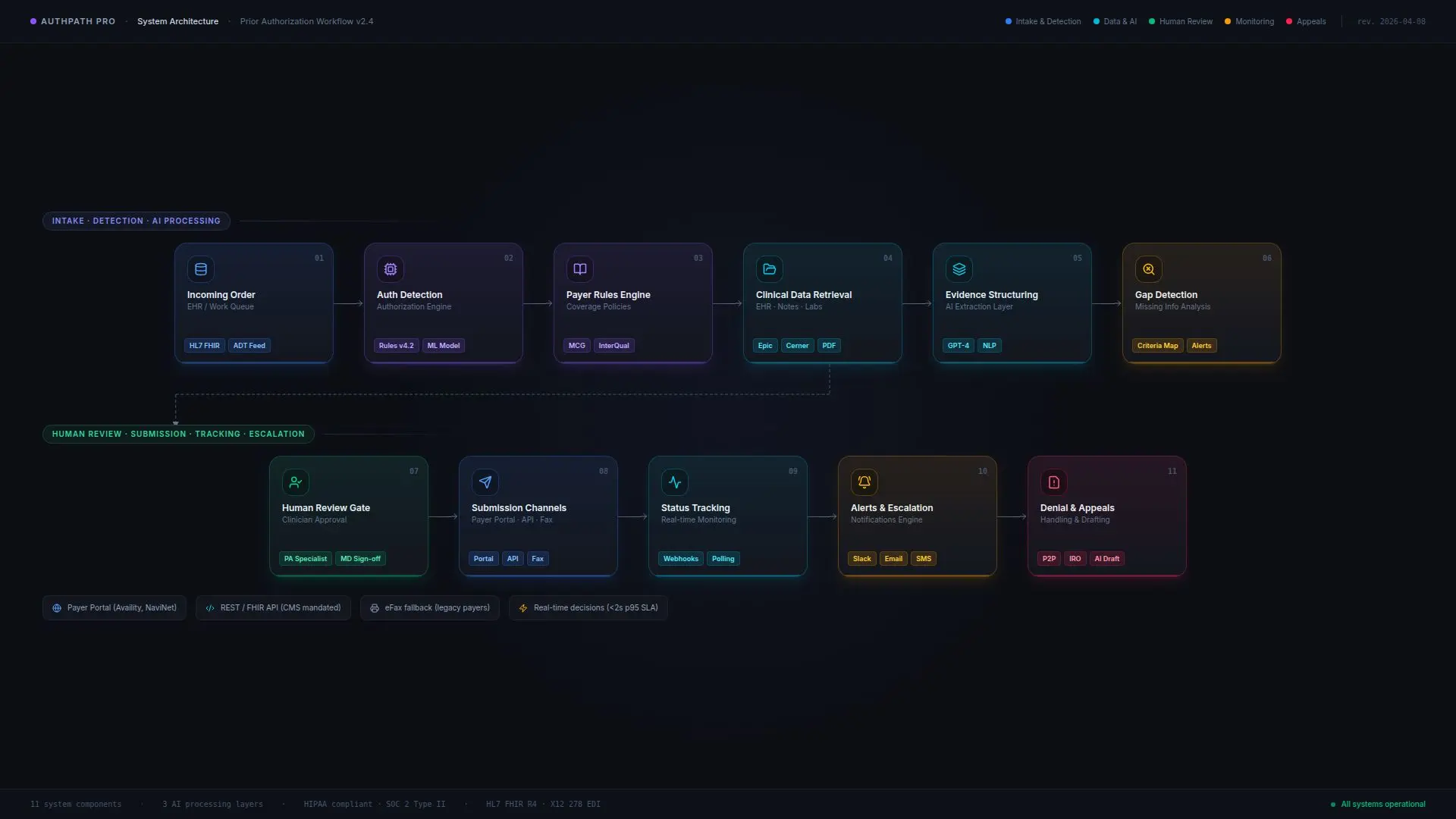
The Solution
Detect authorization requirements from incoming orders and work queues
Gather relevant clinical documentation from the EHR and related sources
Structure the evidence into payer-specific submission formats
Identify missing information before submission
Assist staff with justification packets and follow-up requests
Track authorization status across channels
Trigger reminders and escalation workflows when timeframes were at risk
Prepare draft appeal materials for denied requests
Maintain a complete audit trail across the workflow
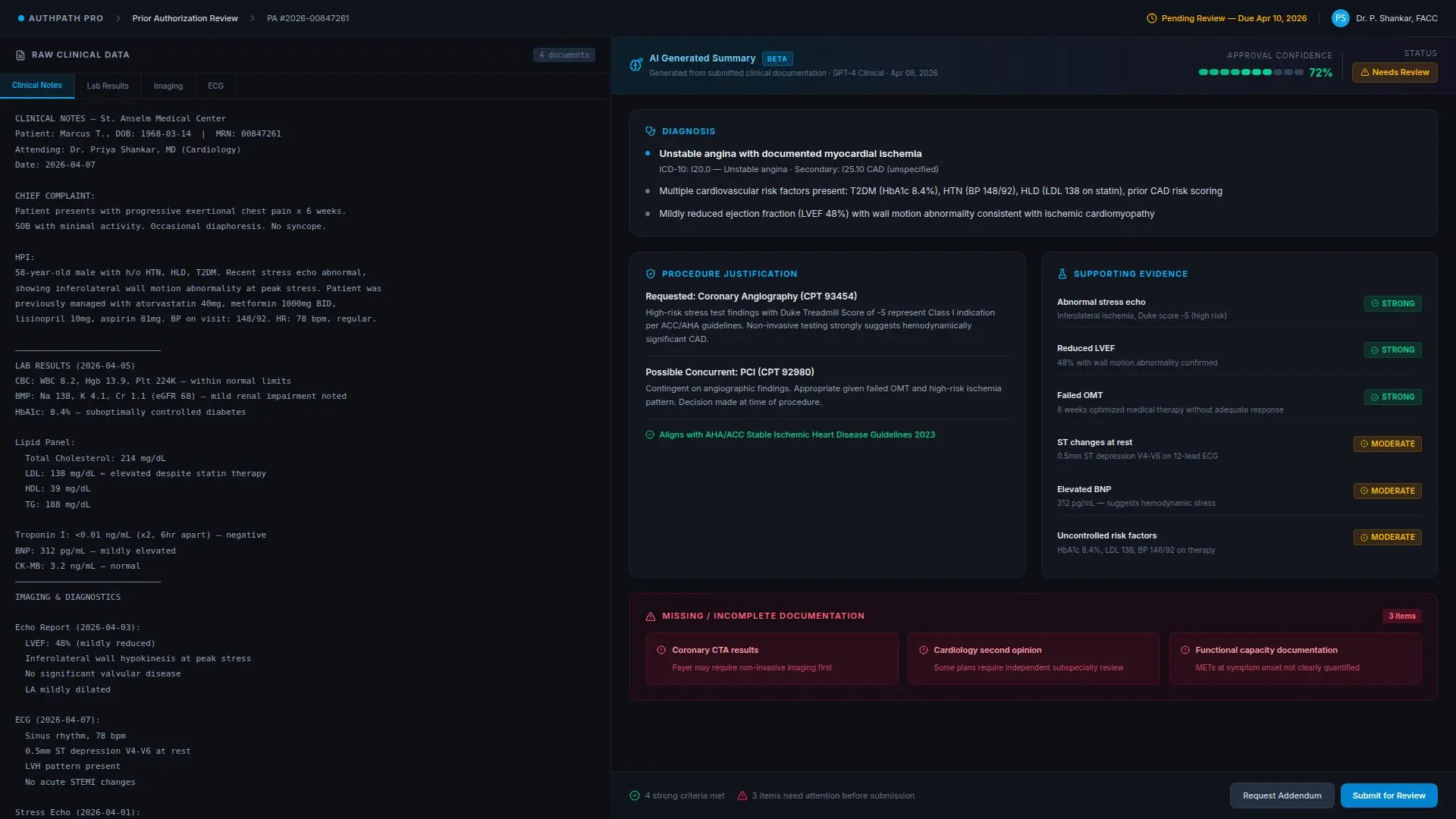
What the System Actually Did
When a prior authorization request entered the queue, the system did more than create a task. It evaluated the order context, payer rules, and required evidence, then automatically initiated the next steps. For example:
- If a procedure required authorization, the system identified the payer and the likely submission requirements
- It pulled supporting clinical data from notes, results, and structured fields
- It organized those materials into a consistent packet for staff review
- If required documentation was missing, it generated a targeted request instead of forcing staff to discover the gap later
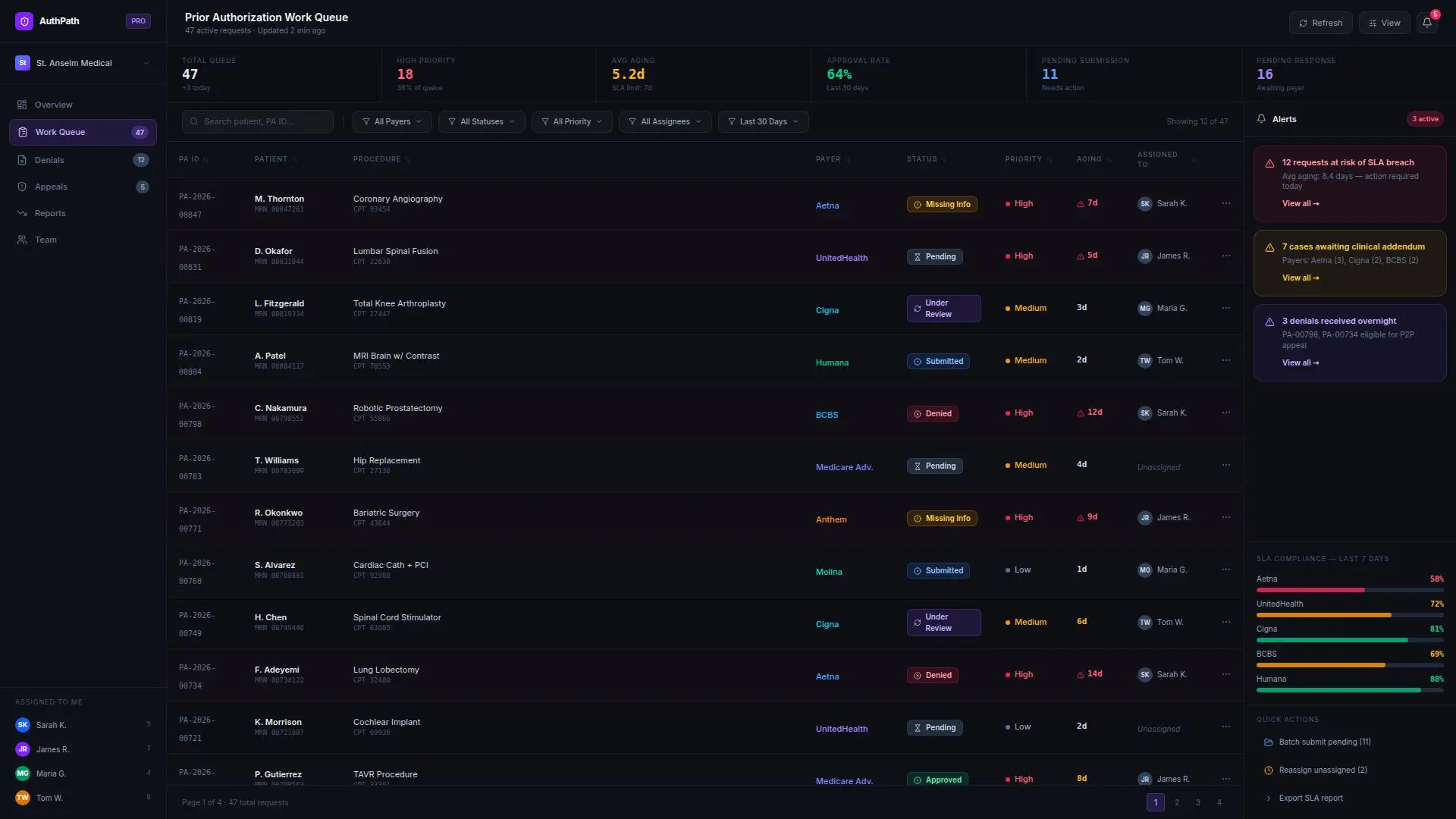
- After submission, it tracked the status and flagged cases likely to miss the required timeframes
- If a denial came back, it prepared a draft appeal summary and supporting evidence package for human review
This is exactly the kind of long-running, exception-heavy workflow where agentic orchestration outperforms basic automation because the work requires messy inputs, repeated follow-up, multiple systems, and clear human checkpoints.
What Product Management & UX Work
This project was not just an integration effort. A major part of the engagement was product strategy and workflow design. We worked with the client to design:
The authorization work queue experience
Payer-specific submission logic
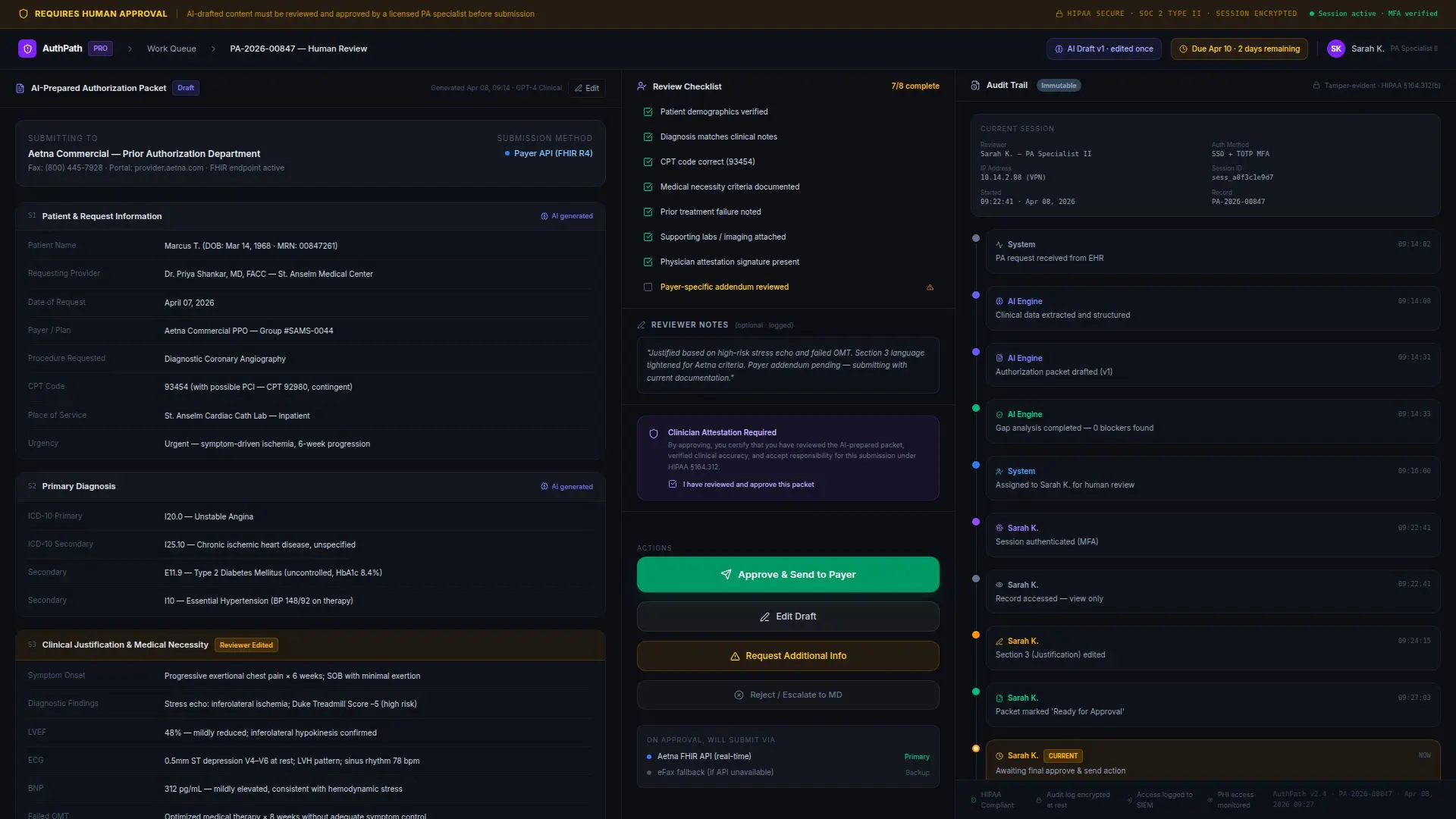
The human review steps before external submission
Staff-facing evidence summaries
Appeal review workflows
Status dashboards for aging requests and exception queues
This mattered because the goal was not simply to automate tasks. The goal was to reduce staff burden without creating a confusing new layer of work. The interface and workflow had to fit the reality of how coordinators, clinic staff, and operations leaders already worked
Security & Controls
Because the workflow touched protected health information and payer communications, the
system was designed with strong controls from the beginning. That included:
Role-based access
Secure handling of PHI
Human approval before high-impact external actions
Logging and audit trails for every workflow step
Clear boundaries between automation, drafting, and final submission authority
Monitoring of system performance and exception handling
That control model aligns with the research guidance around HIPAA, auditability, and bounded autonomy in regulated workflows.
Implementation
The engagement was delivered in stages.
Phase
01
The engagement was delivered in stages
We interviewed teams, mapped current-state workflows, reviewed documentation patterns, and identified the most expensive failure points.
Phase
02
Product and workflow design
We designed the submission workflow, review logic, exception handling, and queue management experience.
Phase
03
System build and integration
We built the orchestration layer, connected it to the client’s internal systems, and implemented structured evidence-gathering, status-tracking, and escalation workflows.
Phase
04
Rollout and training
We launched first with a smaller subset of authorizations, trained staff, refined workflow thresholds, and adjusted based on actual usage patterns.
Phase
05
Monitoring and continuous improvement
After launch, we tracked submission quality, turnaround time, escalation rates, and denial-related rework to improve performance over time.
Results
● improved patient scheduling readiness for authorization-dependent procedures
Just as importantly, authorization staff reported that they were spending less time piecing together paperwork and more time handling true exceptions and payer-specific edge cases.

Why It Worked
This project worked because the system was designed around a real operational bottleneck — not around a generic AI use case.
Prior authorization is one of the clearest examples of where healthcare organizations lose time to manual coordination, incomplete information, and fragmented tools. It is repetitive, measurable, high-volume, and tightly connected to both patient care delays and administrative costs.
The system created value by:
- Reducing documentation friction
- Improving consistency
- Keeping humans involved where judgment mattered
- Making the workflow easier to manage at scale
- After submission, it tracked the status and flagged cases likely to miss the required timeframes
- If a denial came back, it prepared a draft appeal summary and supporting evidence package for human review
Client Outcome
The client did not just get a faster authorization process. They got: